Caught in institutional logic: Swedish public-health campaigns targeting migrants
It is a windy but sunny day in early May 2021. Fatuma approaches an elderly woman who sits on a bench with a crutch in her hands. We are in one of the so-called socially vulnerable areas of Stockholm with low economic status and a high proportion of people with a migration background. The women speak a non-European language, and we see Fatuma handing out a piece of paper. In the voiceover, Fatuma explains that she works as a hälsoinformatör, a health informer, and reaches out to people in the area who don’t watch Swedish news. She talks to them about the vaccination programme that is being rolled out in Sweden and how to book a vaccination time. So begins a news report that was broadcast on Swedish television on 4 May 2021.
Public health information for migrants: More than translations
The vignette illustrates a specific instance of an information campaign about public health in a multilingual setting. Fatuma hands out a flyer, presumably with information on how to get vaccinated written in a language that is not Swedish. Importantly, she engages in dialogue with the women, answers questions and explains. Fatuma thus makes the abstract information on the flyer relevant for the women she meets. As a temporal employee of the council who is knowledgeable about the vaccination campaign and as a resident in the area who speaks relevant languages besides Swedish, Fatuma can mediate between the abstract discourse of the public information and the situated discourse of the interaction. While she calls herself a health informer, her mediation work can be seen as health brokering.
Health informers like Fatuma were first employed in the spring of 2020 when it became clear that people with lower socio-economic status and living in certain vulnerable areas (often correlated with being born outside of Sweden) had higher risks of contracting Covid-19, of needing intensive care and dying due to the viral disease[1]. In the spring of 2021, health informers were called on again when it became clear that the vaccination rate among these communities was significantly lower compared to the national average[2]. Since 2010, a number of projects have engaged health informers to reach out to people with migration backgrounds living in Greater Stockholm[3]. The overarching aim has been to reduce health inequality, i.e. the systemic differences in health between social groups with different social positions in a country[4]. Similar mediation work has been identified as a success factor in previous health communication campaigns[5].
These efforts suggest that simply translating information into minority or migrant languages is not enough to encourage changes in people’s behaviour, or in the most recent case, getting vaccinated. But why would this be the case? And why do we still bother with printing translations? Maybe we need to take a closer look and reconsider what information giving and receiving means for different stakeholders.
Looking at institutional communication practices from the inside
This blog post aims to examine institutional communication practices from the inside – at the levels of designing printed information and distributing it. Based on a study of a health-information campaign from 2015/16, I discuss the tensions between the institutional aim to influence the behaviour of specific social groups through communication and the practical needs of these people. I thus consider health governance through the lens of practice theory.
My motivation for writing this blog is to provide additional perspectives on institutional communication directed at multilingual audiences in situations of crisis, i.e. situations that threaten the smooth running of the public health service. It is a response to criticism which either dismisses such institutional campaigns as ineffective due to translation issues or a lack of receptiveness on the side of the audience. I want to raise awareness of the complexity of institutional communication in its design and distribution. An additional aim with this blog is to emphasize the need to refrain from grant narratives and quick generalizations, and instead open up for multiple narratives and (in the spirit of this blog site) slow research.
Before I commence, I briefly outline the context of health communication in Sweden, and introduce the study. I will then present relevant findings and reflect on implications for understanding the current campaign related to the Covid-19 pandemic.
The Swedish public healthcare system and health communication
Sweden has a public healthcare system in which the responsibility for healthcare provision lies with its 21 regional councils. This means that for instance the regional council in Greater Stockholm (Stockholm Regional Council) is responsible for distributing the vaccine and offering vaccinations throughout its 26 local municipalities. Since the local municipalities are responsible for areas such as schooling, care for the elderly and social services for asylum seekers, they cooperate in the rolling out of the vaccination programme. Both regions and local municipalities are governed by elected bodies, and their respective administrative units are responsible for operationalizing political directives.
Swedish legislation stipulates that healthcare provision should allow equal access for all inhabitants[6]. Health equity, i.e. aiming for equal results with regards to health and quality of life across the population[7], is a central tenet of the Swedish welfare state. Besides providing the means, informing about ways to access this provision is a central task of the regional councils. In the current pandemic, a number of specialised national (first and foremost the Swedish Public Health Agency, the Swedish Civil Contingencies Agency) and regional (e.g. the Infectious Disease Unit Stockholm) agencies have been involved. But most of the printed and digital material has been developed under the oversight of the regional councils. In this blog I will therefore focus on information campaigns on the regional level and the example of Stockholm Regional Council.
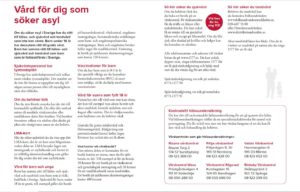
© Stockholm Regional Council, Nov 2015, see Kaufhold and Wirdenäs, 2018
Public health-information design and distribution: The 2015/16 campaign
To unpack the complexity of public health communication, I will now turn to a study which investigated a communication campaign about access to healthcare for newly arrived migrants[8]. In this study, my colleague Karolina Wirdenäs and I identified tensions between the institutional aim of influencing the behaviour of the newly arrived migrants through information giving and the practical needs of these people.
The campaign was rolled out during the so-called refugee crisis in 2015/16 in Greater Stockholm. In this period unprecedented numbers of asylum seekers and migrants in transit arrived in Sweden. Due to their hazardous journeys, they were often in need of healthcare. The aim of Stockholm Regional Council was to address these needs, while avoiding over-burdening parts of the healthcare system, such as emergency departments. The Council therefore produced brochures and posters to inform the newly arrived migrants about their right to receive some healthcare and ways to access healthcare. This material was sent out to local municipalities, NGOs/charities and healthcare providers, who were asked to distribute the brochures amongst the migrants.
Similar to the current campaign, mediation became an important aspect. Our study reveals some factors at the level of designing information material that hindered public information to be effective. At the level of distributing this material, our findings highlight the need to recontextualize the information into the lifeworlds of the newly arrived persons.
Studying institutional communication through text analysis and retrospective interviews
We studied the campaign retrospectively in 2017 and worked as independent researchers closely with the council. Through our contact person at the council’s communication office, we gained access to the material that had been sent out from November 2015 onwards, and to the recipients.
We first analysed the printed material. To understand the production process, we interviewed staff at the county council who had been involved in the design. To gain insights into the distribution and use of the material, we interviewed representatives of the different recipient groups (13 participants in total). In addition, we interviewed an asylum seeker with prior medical training as a representative of the target audience for the brochures.
Designing health-information: The printed material
Let’s have a closer look at the brochures. The intention was that these brochures would be handed out to migrants by staff and volunteers in clinics, municipality offices and accommodation centres. Therefore, each version included the information in Swedish and two other languages (English, Arabic, Tigrinya or Dari).
What can we say about the design of the brochures? The figure at the top illustrates the layout of the text. The information was organized in topical chunks under sub-headings. Spaces between the short paragraphs allowed easy access to information. The text informed about rights, legal requirements and access to healthcare. Despite the intended wider audience (staff and volunteers), the text explicitly identified asylum seekers as readers.
At the same time, the text presupposed substantial knowledge about the Swedish healthcare system, which someone who has just arrived in Sweden is unlikely to know. For instance, what is the meaning of a statement like “children have the same right to healthcare and dental care as children who reside in Sweden”? What rights do the Swedish residents have? Another example is: “you should book a visit at a medical centre”. Is this a suggestion or an obligation? And is a “medical centre” different from an emergency department at a hospital? The use of direct address (you) and formulations that can be understood as invitations rather than requirements are typical for language use in official communication in Sweden. However, in the given context, these relational and face-saving communicative strategies might lead to misunderstandings.
In short, the text was explicitly directed at the newly arrived migrants. Yet to understand it, a mediator was required who was familiar with the organization of the Swedish healthcare system and was able to explain it. Ideally this person would have some understanding of other healthcare systems to mediate between ways of accessing healthcare in different national contexts.
Designing health-information: The production process
So, what did the producers at the regional council say? The most surprising finding was that they were highly aware of the communicative obstacles in the text. We learned that the text formulation was a process that involved existing documents and the consultation of several specialists including lawyers and medical advisors. The producers highlighted a range of challenges, namely: involving all experts within the limited time available; accessing translation services; checking the quality of the translations; and communicating complex information on access under specific legal and medical conditions succinctly and legally sound.
The logic of institutional practices
We witnessed a great willingness to help and facilitate access to healthcare from all sides. Some of the council’s administrative staff even helped as volunteers in their leisure time. Yet their reasoning around their professional communication activities positioned them within the logic of institutional practices.
Following the philosopher of practice theory Theodore Schatzki[9], practices are organized constellations of activities, including discursive activities. According to Schatzki, practices are organized alongside four interrelated dimensions: practical understandings (the know-how of producing the brochure), explicit rules (policies and guidelines for state communication), teleoaffective structures (aims, beliefs and expectations with regards to what the texts can achieve), and general understandings or discourses (such as the value of health equity and the ideal of the Swedish welfare system).
Applied to the production practices, we see that the producers had the know-how of designing brochures in terms of layout and text formulations. The interview revealed that they had started from existing texts and did not consult guidelines about the use of clear Swedish in public communication (e.g., addressing the reader directly as “you”). Instead, they drew on their experience from previous instantiations of the practice.
In terms of rules and guidelines, they emphasized the requirement to involve various specialists and ensure that the text is legally sound. It was important to be correct even if this might make the text more difficult to read. They described this tension as “a continuous fight between what is correct and what is easy to read”.
The producers formulated various aims that they associated with the texts. The primary goal was to provide a quick reference guide for Swedish-speaking staff and volunteers as well as for migrants. They also expressed the intention of “steering behaviour”. For instance, they suggested that the sequence of the information given would lead people to contact appropriate healthcare providers and avoid overloading others.
These aims reflect some general understandings that we can also identify in debates around healthcare provision in the current pandemic situation. There was of course the intention to help and enable access to healthcare. Steering behaviour was to ensure that available resources within the Swedish healthcare system were used in the best way. In practical terms, the aim was to redirect patients from accessing emergency departments to clinics that could deal with less severe issues. The discourse of the efficient use of resources is well-documented in relation to the Swedish welfare system[10] and it recurred in all stakeholder groups.
Distributing health-information: The brochures became artefacts
The brochures were distributed widely among the stakeholder groups that included local municipalities, NGOs/charities, civic or religious associations, and the healthcare providers in the Greater Stockholm. Thus, the communication office at Stockholm Regional Council pragmatically used existing contacts of groups they had worked with before. Several interviews indicated that the material did end up in the hands of migrants. Yet the recipients had different information needs. Some of the healthcare professionals reported that they had consulted the material in combination with other online sources to inform themselves. Others explained that they already had detailed knowledge about medical requirements and access rights.
In our interviews, it became clear that the main value of the brochures was symbolic. Besides providing some contact information and links to further resources, they constituted artefacts to hand out. The complex general content did not help to solve practical issues that needed to be addressed there and then. For instance, while the brochure introduces the right to an interpreter, there was not always time to find and arrange a suitable interpreting service. Instead, a doctor or nurse who spoke a relevant language helped out. Similarly, the brochure suggested that asylum seekers have the right to access some healthcare. Yet there were many migrants in transit or without documents, who did not apply for asylum in Sweden. Validating that they also had the right to some healthcare often involved asking specialist healthcare professionals.
Going beyond the logic of institutional practices
The uniqueness and limitations of the institutional practices become clearer when we compare them to the NGO stakeholder. In the interview, a representative of an NGO positioned their work as advocates for migrants’ rights to access healthcare. This involved supporting migrants – based on their legal and medical knowledge – and explaining migrants’ health needs to the regional council – based on their first-hand knowledge of the situation in 2015/16 “out there in the reception centres”. In fact, they suggested that they partly encouraged the regional council to send medical staff to the reception centres rather than waiting for persons in need of healthcare to figure out which type of healthcare service to access.
The producers and the NGO we interviewed shared the general understanding that available resources within the healthcare system should be used efficiently. They differed in their understanding of how this could be achieved in times of an acute need of healthcare provision. The producers adhered to the institutional logic in which the organizational structures were a given and the behaviour of patients had to be corrected. The NGO, on the other hand, suggested a modification of the organization (by sending out healthcare practitioners) to make the system work in the exceptional situation of 2015/16. Having said this, the NGO did distribute the brochures and regarded them to be an important additional source of information. Collaboration with the council is an important part of their work, but this also includes demanding further action from the council if necessary.[11]
Overcoming limitations by recontextualizing information
I stated above that the information in the brochure required mediation and recontextualization. All stakeholders suggested that they had been involved in some form of mediation. In their role as mediators, they recontextualized information, i.e., they had to relocate and thereby transform official information to fit the current communicative situation[12]. They drew on the information in the brochures and searched for further information to be able to deal with the issues they encountered. To be able to explain how the healthcare system in Sweden works, it was advantageous to understand differences between healthcare systems. At this level, the mediation resembled cultural brokering, which involves not only translating between languages but also between cultural contexts[13] and associated discourses[14]. Professionals who mediate health information in the sense of cultural brokering are known as health brokers[15].
Reflecting on the current vaccination campaign
Similar to the 2015/16 campaign on access to healthcare, the current campaign about vaccination aims at influencing people’s behaviour. Presumably, the printed campaign material was produced in similar ways as the material for the access to healthcare campaign. Either due to learning from the previous campaign or due to the different message, the information is substantially shorter (one or a few phrases) and less complex. But again, we see practical obstacles[16]. For instance, while the information on hygienic behaviour might be less complex than information on accessing the Swedish healthcare system, keeping a distance might not be so easily achievable (or meaningful) in areas with overcrowded housing. Moreover calls for booking a vaccination time are difficult to follow for some if the automatic phone reply first offers a range of options in Swedish (or English) or if the booking app requires hard- and software that might not be accessible for all (Raili Marling discusses digitalization of health care services in Estonia).
A major difference between the campaigns is that the information campaign about Covid-19, which targeted people living in socially vulnerable areas, moved to some extent beyond the established institutional structures. It involved local stakeholders in the design phase and designated mediators in the distribution phase. The translated information material for these groups was distributed relatively late, but the work intensified once the authorities had received reports that there were higher proportions of Covid-19 patients from these areas. Local actors in these areas, such as the municipalities and civic and religious associations, were involved in the design of the campaign[17]. The first health informers started their work on 18 March just after the first translated printed material had been launched[18].
Health informers as official mediators seem to have gained a more central role. These health informers not only speak relevant languages, but they usually also live in the area. Supported by the regional council they regularly update themselves on scientific information about the virus and the vaccines. The information from the Public Health Agency is the essential source of information, and health informers like Fatuma recontextualized this information in conversation with the citizens they meet in these areas. But most importantly, mediation involves building trust as Fatuma explained at an open seminar organized by the regional council on 10 November 2021. Health informers need to be able to listen and engage in dialogue. While trust building was relevant in the access-to-healthcare campaign in terms of the healthcare system and its principle of confidentiality, now the reliability of the information is essential.
The most recent statistics on vaccination rates show that there are still lower rates in socially vulnerable areas compared to the Swedish average. This observation is supported by the Public Health Agency’s most recent survey[19] on the acceptance of the vaccination against Covid-19 among Swedish residents who were born in Middle Eastern and African countries. While these results cannot be directly related to the work of the health informers in Greater Stockholm, they provide a basis for informed speculation. The report suggests that the proportion of respondents with a positive attitude towards vaccination was higher among older participants. In contrast to previous surveys, there was no significant difference correlating with the length of the participants’ stay in Sweden. The multilingual information campaign was, in the first instance, directed at people with low proficiency in Swedish, which might include those who recently arrived in Sweden and older persons who might not use Swedish regularly. Finally, the report confirms a trend that the proportion of vaccinated people is higher among those with a university-level education. This might indicate further structural differences that the information campaign has not addressed. The relation between structural differences in the form of socio-economic status has been debated in the public health context of Sweden in terms of health equity for some time, and the pandemic has highlighted this issue[20]. When it comes to the design of information campaigns for multilingual groups of inhabitants living in specific areas, the comparison indicates some development. Going beyond translations and involving communities (as an additional expert group) seems to have been recognized as an important factor for making the message meaningful for its target audience.
[1] Public Health Agency. (2021a). Utrikesfödda och Covid-19 Konstaterade fall, IVA-vård Och Avlidna Bland Utrikesfödda i Sverige 13 Mars 2020 – 15 Februari 2021. (Artikelnummer: 21051). www.folkhalsomyndigheten.se/publicerat-material
[2] As an example from April 2021 we can compare the group of people aged 80 or older. Of these, 91% of the Swedish-born population were vaccinated at that time but only 59% of those born in North Africa and 44% of those born in sub-Saharan Africa. Source: Public Health Agency. (2021b). Covid-19 vaccinationstäckning och födelseland. (Artikelnummer: 21102). https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/c/covid-19-vaccinationstackning-och-fodelseland-/?pub=92033.
[3] Bäärnhielm, S., Hussein, H., Baker, U., & Allebeck, P. (2013). Hälsokommunikatörer Kan Bidra till Bättre Hälsa hos Utlandsfödda. [Health brokers can contribute to better health of people born abroad.] Läkartidningen, 110(CAZZ), 1-3.
[4] Swedish Commission for Equity in Health. (2016). Det handlar om jämlik hälsa: Utgångspunkter för Kommissionens vidare arbete. Delbetänkande av Kommissionen för jämlik hälsa. SOU 2016:55. Stockholm. http://kommissionjamlikhalsa.se/wp-content/uploads/2016/08/det-handlar-om-jamlik-halsa_sou-2016_55.pdf
[5] Kaufhold, K., & Wirdenäs, K. (2018). Att mediera information om vårdmöjligheter för nyanlända: Evaluering av SLL:s kommunikation 2015/16. Slutrapport. Stockholm: Stockholms läns landsting och Stockholms universitet. http://urn.kb.se/resolve?urn=urn:nbn:se:su:diva-155535
[6] Healthcare Act. (2017:30). https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/halso–och-sjukvardslag_sfs-2017-30
[7] Sandman, L. (2017). Att prioritera i vården: en etisk nödvändighet. Evidens, 2, 4-8. https://janusinfo.se/download/18.10adba9e1616f8edbc924a75/1535626560941/Evidens_nr2_2017.pdf
[8] Kaufhold, K., & Wirdenäs, K. (2021). Professional identity construction in the healthcare sector: Narratives around facilitating migrants’ access to healthcare. Journal of Applied Linguistics and Professional Practice, 15(2), 163-186. https://doi.org/10.1558/jalpp.20369
[9] Schatzki, T. R. (2002). The site of the social: A philosophical account of the constitution of social life and change. Pennsylvania State University Press.
[10] Petersson, J. (2012). From medicine by wire to governing wireless: Changing geographies of healthcare. In B. Larsson, M. Letell, & H. Thörn (Eds.) Transformations of the Swedish welfare state (pp. 153–167). Palgrave Macmillan.
[11] For more detail, see Kaufhold and Wirdenäs 2021, endnote 8.
[12] Cf. Linell, P. (1998). Discourse across boundaries: On recontextualizations and the blending of voices in professional discourse. Text, 18(2), 143-157.
[13] To be clear, culture is understood here as differences in practices and/or worldviews.
[14] Papen, U. (2010). Literacy mediators, scribes or brokers? The central role of others in accomplishing reading and writing. Langage et société, 133(3), 63-82.
[15] See e.g. Torres, S., Labonté, R., Spitzer, D.L., Andrew, C., & Amaratunga, C. (2014). Improving health equity: The promising role of community health workers in Canada. Healthcare Policy, 10(1), 73-85.
[16] Aside from the issue that usually more than verbal appeals are needed to change human behaviour effectively. See: Shove, E., Pantzar, M., & Watson, M. (2012). The dynamics of social practice: Everyday life and how it changes. Sage.
[17] KPMG. (2021). Region Stockholms hantering av Covid-19. Oberoende utvärdering av perioden 1 Januari 2020 till 31 December 2020. [Stockholm Regional Council’s handling of COVID-19. Independent evaluation of the period 1 Jan – 31 Dec 2020] https://www.regionstockholm.se/globalassets/5.-politik/politiska-organ/regionfullmaktige/2021/2021-05-04/20210504/p-25-oberoende-utvardering—sekretessprovad-2021-03-09.pdf
[18] KPMG. (2021). Region Stockholms hantering av Covid-19. Oberoende utvärdering av perioden 1 Januari 2020 till 31 December 2020. [Stockholm Regional Council’s handling of COVID-19. Independent evaluation of the period 1 Jan – 31 Dec 2020] https://www.regionstockholm.se/globalassets/5.-politik/politiska-organ/regionfullmaktige/2021/2021-05-04/20210504/p-25-oberoende-utvardering—sekretessprovad-2021-03-09.pdf
[19] Public Health Agency. (2021c). Acceptans för Covid-19-vaccination: Invånare i Sverige födda i Afrika och Mellanöstern. (Artikelnummer: 21244). https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/a/acceptans-for-covid-19-vaccination-del2/?pub=102025
[20] Public Health Agency. (2022, March 24). Skillnader i livsvillkor påverkar folkhälsans utveckling. https://www.folkhalsomyndigheten.se/nyheter-och-press/nyhetsarkiv/2022/mars/skillnader-i-livsvillkor-paverkar-folkhalsans-utveckling/
How to cite this blog post:
Kaufhold, Kathrin (2022), “ Caught in institutional logic: Swedish public health campaigns targeting migrants „, Crisis Discourse Blog (CriDis), URL = https://www.crisis-discourse.net/de/2022/06/swedish-public-health-campaigns-targeting-migrants/.